Vitamin B12 — Structure, Food Sources, Benefits, and Deficiency

Introduction
Vitamin B12 is a water-soluble vitamin naturally present in several foods, mainly of animal origin. The vitamin is also added to some foods and is available as a dietary supplement and a prescription medication.
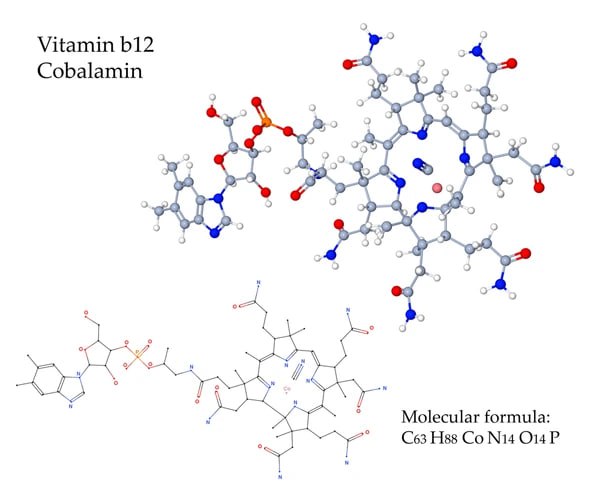
Vitamin B12, or cobalamin, contains the mineral cobalt, which is responsible for its red color. Cobalamin is considered one of the most complex nutrients in terms of structure and function in the body.
Table of contents
- Structure
- Absorption & Metabolism
- Physiological Role in the Body
- Recommended Intakes
- Vitamin B12 Synthesis & Food Sources
- Vitamin B12 & Human Health: Benefits & Risks
- Inflammation and Oxidative Stress
- Cancer
- Cardiovascular Health & Stroke
- Cognitive Function and Dementia
- Osteoporosis
- Vitamin B12 Deficiency: Causes, Symptoms, & Pathogenesis
- Adverse Drug Reactions
- Interactions With Medications
- Special Considerations
- Historical Background of Vitamin B12
- Summary
- References
Structure
Cobalamin (C63H88CoN14O14P) consists of a corrin ring with a central cobalt(III) ion, surrounded by four nitrogen atoms from pyrrole groups, separated evenly and directly across each other, connected by a methylene link on the other sides and possessing seven amide side chains. Additionally, cobalamin has a fifth nitrogen coming from 5,6-dimethylbenzimidazole indirectly connected to the cobalt ion and a ribose sugar (five-carbon sugar) linked to a nucleotide phosphate group.
Absorption & Metabolism
Vitamin B12, or cobalamin, is bound to a protein in food and released before absorption. In the stomach, hydrochloric acid (HCl) and gastric protease separate vitamin B12 from its protein bond, and the freed vitamin B12 binds with haptocorrin, a cobalamin-binding protein or R-protein, secreted by salivary and parietal cells (oxyntic cells). Haptocorrins protect the vitamin from chemical changes. Duodenal digestive enzymes and pH change free the vitamin from haptocorrin and trigger the transfer to intrinsic factor, a protein secreted by the stomach’s parietal cells. This complex is absorbed in the most distal part of the small intestines - the distal ileum, by receptor-mediated endocytosis (1, 2). Finally, lysosomal enzymes free vitamin B12 from the complex to let it bind to transcobalamin II. Bound to transcobalamin II, vitamin B12 travels directly to target organs (3).
Vitamin B12 fortified foods and dietary supplements contain the vitamin in its free form; thus, the separation step is skipped during absorption (1).
The two biologically active forms of vitamin B12 are 5-deoxyadenosylcobalamin (Ado-Cbl) and methylcobalamin (Met-Cbl). The two other forms of vitamin B12 - cyanocobalamin (CN-Cbl) and hydroxocobalamin (OH-Cbl) are converted to the vitamin’s active forms inside the body (1).
Physiological Role in the Body
The primary metabolic function of vitamin B12 is its cofactor role for two enzymes: methionine synthase and L-methylmalonyl-CoA mutase (MCM).
In the cytoplasm, methylcobalamin (Met-Cbl) acts as a cofactor for methionine synthase in the folate-dependent methylation of homocysteine to methionine, which is further metabolized to S-adenosylmethionine. The methylations are required to synthesize myelin, phospholipids, proteins, and neurotransmitters. Impaired methylation leads to neurological consequences. Methylcobalamin is also essential for folate conversion (methyltetrahydrofolate to tetrahydrofolate), which is required for the synthesis of purines and pyrimidines, organic compounds required for DNA and RNA production. Thus, untreated vitamin B12 deficiency will impair DNA synthesis and lead to megaloblastic anemia development.
In the mitochondria, 5-deoxyadenosylcobalamin (Ado-Cbl) acts as a cofactor for MCM, catalyzing the reversible isomerization of L-methylmalonyl-CoA to succinyl-CoA. This reaction is required for the catabolism or breakdown of ketogenic amino acids, odd-chain fatty acids, and cholesterol. The absence of Ado-Cbl causes either accumulation of methylmalonic acid or methylmalonic aciduria; both are linked to impaired myelination and cognitive functioning (4, 5).
Due to its chemical stability, cyanocobalamin (CN-Cbl) is convenient for medical use. Hydroxocobalamin (OH-Cbl) is used as an antidote for cyanide poisoning (1, 3).
Recommended Intakes
According to the 2020-2025 Dietary Guidelines for Americans, the recommended daily value (RDV) of vitamin B12 for adults is 2.4 mcg (6).
The table below shows the RDV of the vitamin for people of all age groups; there is no difference between the sexes (6).
| 2-3 years | 4-8 years | 9-13 years | 14-18 years | 19-30 years | 51+ years |
| 0.9 mcg | 1.2 mcg | 1.8 mcg | 2.4 mcg | 2.4 mcg | 2.4 mcg |
Vitamin B12’s circulation concentrations reach their highest level about seven hours after supplement administration. Vitamin B12’s half-life in plasma is approximately six days, whereas in the liver, it's approximately one year (7). The body stores 2-5 mg of vitamin B12, half of which is in the liver (8).
Vitamin B12 Synthesis & Food Sources
Vitamin B12 is synthesized only by certain bacteria and archaeons. The microorganisms can be found in soil, water, and animals’ stomachs. The synthesized vitamin B12 accumulates in animal tissues, particularly the meat and milk of herbivorous ruminant animals (e.g., cattle, sheep, and sheep).
In aquatic environments, most phytoplankton acquire vitamin B12 through a symbiosis with certain bacteria, and then fish and shellfish consume the phytoplankton.
Edible plants and mushrooms may also contain some vitamin B12, mainly due to the bacteria in the soil or their aerial surfaces (9).
The table below shows the primary dietary sources of vitamin B12 and their concentration per 100g serving of each product.
| Clams, mixed species | 98.9 mcg |
| Beef liver | 70.58 mcg |
| Caviar, black and red, granular | 20 mcg |
| Salmon | 2.8 mcg |
| Beef, ground, 85% lean meat | 2.64 mcg |
| Tuna | 2.35 mcg |
| Meckerel | 19 mcg |
| Pork liver | 18.67 mcg |
| Oysters | 17.5 mcg |
| Crab meat | 11.5 mcg |
| Cheddar cheese | 1.1 mcg |
| Eggs | 1.1 mcg |
| Greek yogurt | 0.75 mcg |
| Pork, shoulder | 0.74 mcg |
| Milk | 0.45 mcg |
| Chicken meat | 0.3 mcg |
Varying levels of vitamin B12 can be found in poultry, red meat, dairy products, nutritional yeast, fortified breakfast cereals, and other fortified products.
Vitamin B12 & Human Health: Benefits & Risks
Inflammation and Oxidative Stress
Vitamin B12 possesses antioxidant and anti-inflammatory properties by scavenging reactive oxygen species (ROS). According to many in vitro studies, superoxide ions in the cytosol and mitochondria are reduced in the presence of adequate B12 levels. The scavenging effects are especially strong in the nervous system. Vitamin B12’s antioxidant activities may be due to various effects, including preserving cellular glutathione and converting homocysteine to methionine (5).
Cancer
The evidence between vitamin B12 intake and cancer risk is mixed. Some evidence supports a link between increased cancer risk and high blood concentrations of the vitamin; some supports a link between lower concentrations and increased cancer risk; and finally, some evidence indicates no overall link (1).
Observational evidence supporting the positive association between higher vitamin B12 and increased cancer risk has included an analysis of data on over 750,000 people with a median age of 56 years. The results indicate a positive correlation between high plasma concentrations of vitamin B12 and an increased cancer risk within a year. Another analysis of 25,000 people with diagnosed cancer found that higher plasma vitamin B12 concentrations have a greater impact on one-year survival rates: 35.8% in those with >1,084 pg/mL and 69.3% in those with 271-813 pg/mL vitamin B12 plasma levels.
A cohort study on over 75,000 middle-aged participants found that ≥55 mcg/day of supplemental vitamin B12 for ten years was associated with a 40% higher risk of lung cancer in men but not women. Other observational studies found no associations between vitamin B12 intake and pancreatic, breast, esophageal, or stomach cancer risks.
A meta-analysis of 18 clinical trials, including approximately 74,500 individuals, found no association between daily 20-2,000 mcg of vitamin B12 intake and cancer risk or all-cause mortality during 2-7.3 years follow-up periods.
In contrast, evidence suggests that low serum vitamin B12 levels are associated with an increased risk of stomach cancer, especially in male smokers. Two meta-analyses found associations between low vitamin B12 levels and increased colorectal and prostate cancer risks (1).
Cardiovascular Health & Stroke
Low vitamin B12 levels lead to elevated homocysteine levels, which, in turn, has been associated with an increased risk of cardiovascular disease. Researchers have hypothesized that supplementation with vitamin B12 and other micronutrients involved in homocysteine metabolism may reduce the risk of heart disease.
However, studies have found negative associations between B12 intake and cardiovascular disease risks. Two meta-analyses, including over 750,000 people (5000 developed coronary heart disease and 10,749 developed stroke), found no significant association between vitamin B12 intake and heart disease risk. Clinical trials also suggest vitamin B12 and folate supplements lower homocysteine levels only, but not heart disease risks.
The authors of a Cochrane Review on this topic have concluded that supplements of vitamin B12 alone or with other B vitamins do not prevent heart attacks or reduce heart-related death rates (1).
Cognitive Function and Dementia
Observational studies have found a link between elevated homocysteine levels and the incidence of both Alzheimer’s disease and dementia. According to a hypothesis, elevated homocysteine levels might negatively affect the brain due to various mechanisms, such as cerebrovascular ischemia leading to neuronal cell death, activation of tau kinases leading to tangle deposition, and inhibition of methylation reactions (1).
Most observational studies have found correlations between low plasma vitamin B12 levels alone or combined with high folate levels and impaired cognitive function. An analysis of cross-sectional 2011–2014 NHANES data found that cognitive impairment risk may be increased by two to three times when low levels of vitamin B12 are combined with high folate or vitamin B9 levels. However, several studies have found no such associations. Additionally, according to a systematic review of over 14,000 participants followed for 5.4 years, the evidence does not support a role for low vitamin B12 levels in the development of cognitive impairment or dementia.
Evidence from clinical trials shows that vitamin B12 supplementation for up to 10 years does not improve cognitive function in older adults with or without dementia, cognitive impairment, or Alzheimer's disease. Similarly, supplementation with vitamin B12 or B-complex vitamins may not decrease the risk or slow the progression of dementia or Alzheimer’s disease in older adults (1).
Osteoporosis
According to a review of 19 observational studies, 12 found no association between vitamin B12 intake and bone mineral density, bone turnover biomarkers, or fracture risk. The remaining seven studies supported the protective role of the vitamin in preserving bone density and reducing fracture risk (10).
Vitamin B12 Deficiency: Causes, Symptoms, & Pathogenesis
Vitamin B-12 is highly conserved through the enterohepatic circulation; thus, a deficiency from malabsorption develops after 2-5 years, and a deficiency from inadequate dietary intake develops after 10-20 years (8).
Risk Groups
Most causes of vitamin B12 deficiency are listed below (1, 2, 10, 11):
- Malnutrition in vegetarians, vegans, and infants of vegan women
- Obesity
- Stomach and small intestinal disorders, such as atrophic gastritis, autoimmune gastritis, chronic gastritis caused by H. pylori, eosinophilic gastroenteritis, celiac disease, Crohn’s disease, backwash ileitis, tropical sprue, small intestinal bacterial overgrowth, parasitic infestations, radiation enteritis of the distal ileum, lymphoma, tuberculosis, amyloidosis
- Gastrointestinal surgeries, such as weight loss surgery or gastrectomy, ileal resection
- Pancreatic insufficiency, including chronic pancreatitis, autoimmune pancreatitis
- Other autoimmune diseases, such as vitiligo, type 1 diabetes, and autoimmune thyroiditis
- Zollinger-Ellison syndrome
- Inherited disorders, such as intrinsic factor deficiency, Imerslund-Gräsbeck disease, juvenile cobalamin deficiency, genetic polymorphisms encoding transcobalamins, transporting vitamin B12 in the bloodstream or involved in its intracellular metabolism
- Certain medications, such as gastric acid inhibitors, metformin, and nitrous oxide.
Most of the disorders listed above affect one or another step of vitamin B12 absorption, leading to its deficiency. Stomach disorders or surgeries lead to the deficiency of either HCl, intrinsic factor, or both, whereas small intestinal diseases or resections decrease absorption. Pancreatic enzymes are necessary for vitamin B12 to bind to intrinsic factors; thus, pancreatic insufficiency will impair this process.
Pathogenesis
DNA and RNA synthesis, DNA methylation — Vitamin B12 deficiency impairs DNA synthesis, causing cell arrest in the DNA synthesis S phase of the cell cycle, making DNA replication errors, and undergoing programmed cell death.
Hematopoiesis — Hematopoietic precursor cells are rapidly dividing and very sensitive to abnormal DNA synthesis. Vitamin B12 deficiency causes megaloblastic changes due to the slowing of the nuclear division cycle relative to the cytoplasmic maturation cycle, i.e., nuclear-cytoplasmic dyssynchrony. Vitamin B12 deficiency may also lead to ineffective erythropoiesis due to the premature death of the developing precursor cells.
Neuronal function — Vitamin B12 deficiency is known to affect the nervous system adversely, but the exact mechanisms remain unclear. Reduced methylation of neuronal lipids and proteins has been hypothesized to play a role (10).
Symptoms
The hallmark of vitamin B12 deficiency is megaloblastic anemia, characterized by large red blood cells with abnormal nuclei; low counts of white blood cells, red blood cells, and platelets may also be seen.
The symptoms of vitamin B12 deficiency include (1, 11, 12, 13):
- Glossitis (tongue inflammation), mouth ulcers
- Muscle weakness, fatigue
- Palpitations, shortness of breath, headaches
- Pale skin, indigestion, loss of appetite, weight loss, diarrhea,
- Infertility
- Problems with smell or taste, disturbed vision
- Impaired cognition (problems with memory, understanding, and judgment)
- Numbness
- Tingling in the hands and feet
- Trouble walking
- Depression, confusion, irritability, and anxiety.
The mentioned neurological symptoms may occur without anemia, too.
In pregnant and breastfeeding women, vitamin B12 deficiency may lead to neural tube defects, developmental delays, growth problems, and anemia in neonates.
Secondary Folate Deficiency
Vitamin B12 deficiency can result in a secondary or functional folate deficiency known as the methyl-folate trap when folate regeneration (conversion) is impaired, and folate is trapped as 5-methyl-FH4 (14). As previously mentioned, vitamin B12 is essential for folate conversion, which is required for synthesizing organic compounds essential in DNA and RNA production.
Adverse Drug Reactions
Many people receive vitamin B12 supplements without any side effects; however, as with any medication or supplement, it may lead to adverse reactions in some.
Vitamin B12 may cause headaches, dizziness, diarrhea, swelling of the extremities, paresthesia, glossitis, rhinitis, muscle weakness, cramps, pain, extreme thirst, frequent urination, confusion, coughing, fast heartbeat, red skin color on the face, pain, warmth, redness, swelling or tenderness in one leg, hives, rash, itching, difficulty breathing or swallowing (15).
Interactions With Medications
Gastric acid inhibitors, including proton pump inhibitors (omeprazole, lansoprazole, pantoprazole) and histamine 2-receptor antagonists (famotidine, cimetidine, ranitidine), are used in the treatment of peptic ulcer disease, acid reflux, H. pylori infection, and functional dyspepsia. These medications can interfere with vitamin B12 absorption by decreasing the secretion of HCl in the stomach (1, 14).
Metformin, an antihyperglycemic agent, may also reduce the absorption of vitamin B12 and lead to vitamin B12 deficiency. The potential mechanisms include altered intestinal mobility or small intestinal bacterial overgrowth (1, 14).
Nitrous oxide anesthesia can inactivate methionine synthase and MCM, causing deficiency symptoms despite serum vitamin B12 concentrations (14, 15).
Several studies have found a positive association between antiepileptic drugs and cobalamin deficiency, whereas others have found none (14).
Special Considerations
Taking supplements while undergoing chemotherapy is not the best idea, especially for breast cancer patients. A small study found that breast cancer patients who took antioxidants, iron, vitamin B12, and omega-3 fatty acids had worse outcomes than those who did not. People taking the supplements were at a greater risk for breast cancer recurrence and death.
The lead author, Christine B. Ambrosone, PhD, said, "Although this is an observational study and the number of users of supplements was fairly small, the results are compelling. Patients using any antioxidant before and during chemotherapy had an increased risk of their breast cancer returning and, to a lesser degree, had an increased risk of death. Vitamin B12, iron, and omega-3 fatty acid use was also associated with poorer outcomes” (16).
Historical Background of Vitamin B12
The clinical reports and studies of patients with pernicious anemia resulted in enough clinical definition to allow Minot and Murphy to develop the first study on treating the condition in the 19th century, leading them to a Nobel Prize. Even though they were not the first to link the disease with nutritional deficiency, they were the ones prescribing patients with pernicious anemia large amounts of animal liver. They found consistent improvement in the clinical and blood status of all people.
Later, Castle discovered a stomach component missing in pernicious anemia patients, which he called an intrinsic factor. After many years, the intrinsic factor was found to be a glycoprotein, forming a complex with vitamin B12 and promoting its absorption. The vitamin was isolated, crystallized, and characterized in Dorothy Hodgkin’s laboratory, contributing to her Nobel Prize in 1964 (15).
Summary
Vitamin B12, or cobalamin, is a water-soluble vitamin naturally present in several foods, mainly of animal origin. The vitamin is also added to some foods and is available as a dietary supplement and a prescription medication.
The two biologically active forms of vitamin B12 are 5-deoxyadenosylcobalamin and methylcobalamin. The two other forms - cyanocobalamin and hydroxocobalamin (OH-Cbl) are converted to the vitamin’s active forms inside the body.
Vitamin B12 deficiency may lead to megaloblastic anemia, impaired cognition, depression, irritability, anxiety, glossitis, mouth ulcers, fatigue, loss of appetite, problems with smell or taste, disturbed vision, tingling in the hands and feet, and difficulty walking.
Common causes of vitamin B12 deficiency are a vegan diet, atrophic gastritis, autoimmune gastritis, inflammatory bowel disease, weight loss surgery, pancreatic insufficiency, gastric acid inhibitors, metformin, autoimmune diseases, and inherited disorders.
References
- https://ods.od.nih.gov/factsheets/VitaminB12-HealthProfessional/
- https://pubmed.ncbi.nlm.nih.gov/35337622/ https://www.ncbi.nlm.nih.gov/books/NBK546655/
- https://onlinelibrary.wiley.com/doi/10.1002/9783527681754.ch6
- https://www.mdpi.com/2072-6643/15/12/2734
- https://www.dietaryguidelines.gov/sites/default/files/2020-12/Dietary_Guidelines_for_Americans_2020-2025.pdf
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9651173/
- https://emedicine.medscape.com/article/1152670-overview
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5788147/
- https://www.uptodate.com/contents/causes-and-pathophysiology-of-vitamin-b12-and-folate-deficiencies
- https://www.nhlbi.nih.gov/health/anemia/vitamin-b12-deficiency-anemia
- https://www.nhs.uk/conditions/vitamin-b12-or-folate-deficiency-anaemia/symptoms/
- https://www.nhsinform.scot/illnesses-and-conditions/nutritional/vitamin-b12-or-folate-deficiency-anaemia/
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8536822/
- https://www.frontiersin.org/articles/10.3389/fnut.2019.00093/full
- https://pubmed.ncbi.nlm.nih.gov/23183296/
